Introduction
A molecule’s journey from its discovery cradle to the patient’s bedside is highly uncertain and often has a low probability of success. Substantiation of its safety and efficacy to cater to an unmet medical need involves a long span of time and investment of billions of dollars. In order to improve the efficacy of the drug development process, various strategies are designed that aim at eliminating molecules at the earliest stages that do not promise any therapeutic benefit. For a candidate molecule to become a therapeutically benevolent medicine, it is important for it to possess suitable pharmacokinetic (PK) features along with its pharmacological activity.
Some of the vital questions that need to be answered whenever a molecule is advanced towards clinical studies are “Does the molecule have sufficient bioavailability through its intended route of administration? Is the molecule metabolically stable to have sufficient persistence in the human bodies?” In corroboration of this fact, pharmaceutical scientists perform PK screening in the early stages of drug development such that the drugs having unsuitable PK can be eliminated sooner.
Hence, knowledge of the pharmacokinetic behavior of molecules becomes necessary almost as soon as the biological screening of the molecules is performed. Predicting the absorption behavior of a drug in humans in a non-clinical domain involves in vitro tests and in vivo assessment in animals. These studies provide an approximation of the human dosing to be adopted for clinical studies.
Regulatory agencies have made it imperative for the sponsors to submit the pharmacokinetic data of new drug in three animal species prior to its clinical trials. It expects the approximation of pharmacokinetics and pharmacodynamics of a product to be estimated based on studies conducted in animals (usually two rodent and one non-rodent species) (21 CFR 314.610(a)(1)-(4); 21 CFR 601.91(a)(1)-(4)).
In the industrial scenario, due to the limited amounts of candidate molecules and time becoming another limiting factor, screening of molecules for optimal pharmacokinetic properties in the discovery stage can be performed in only one or two animal species. Therefore, the selection of animal species and the experimental design of studies are important in providing a reliable prediction of drug absorption and elimination in humans.
A good compound could be excluded on the basis of results from an inappropriate animal species or poor experimental design. Hence, there subsists the need for models that can help in extrapolating the data from animal studies to suitably predict the human pharmacokinetics with acceptable accuracy and precision.
Another challenge that industry faced was to predict the dose of the patients from the safety studies conducted in healthy human volunteers. The dosing information for various subgroups of patient population like pediatrics, pregnant patients and patients already taking other medications are not supported by sufficient clinical data due to ethical reasons. While the clinical prescription of such drugs would often be off-label, industry has eventually resorted to various mathematical approaches to support the dosing information and hence facilitate the drug approval process.
This also supports the indication of the product in such patient sub-groups as a labeled one. Physiologically based pharmacokinetic (PBPK) modeling is one such approach which has gained wide industrial and regulatory acceptance in the drug development process over other methods like allometric scaling and compartmental modeling.
Physiologically based pharmacokinetic modeling
PBPK modeling is a mathematical approach that intends to create a system based on the compartmentalization of the human physiology into a multiple-compartments ad often ‘lumped’ together based on the common characteristics. The compartments of the system are connected through a common dynamic channel analogous to the blood flow connecting all the organs and glands in a network. As a whole, the system becomes a mathematical description of the average human physiology that has some defining features.
Added to this system are the physicochemical and biological properties of a molecule to predict how the molecule would behave within the system. When the behavior of the molecule in the system is compared and optimized to match the observed clinical pharmacokinetics, the PBPK model becomes complete. Hence, a PBPK model comprises of the parameters related to system and drug (commonly called ‘system-related’ and ‘drug-related input parameters’, respectively). The system-related parameters are independent of the drug but are subject to vary with the patient or patient group. This type of modeling provides us with the conventional PK parameters e.g. half-life, clearance and volume of distribution and most importantly, the concentration-time profile of the drug.
Advantages of PBPK modeling over conventional methods
- PBPK modeling approach possesses factorial power that can be extended to include any other factor that has not yet been considered while developing the model. The model has the intrinsic advantage of integrating new information, both of the system and drug properties to predict the ability of the model.
- Extrapolatory power of the PBPK models helps in predicting the PK from one group of subjects to another based upon known factors of physiology, pathophysiology and the pharmacogenetic variation.
- PBPK modeling describes the journey of the drug within the human physiology both qualitatively and quantitatively. Hence, the assumptions of an optimized PBPK model provide us with the mechanistic insights of the drivers and processes that steer the pharmacokinetics of a drug.
- More predictive than descriptive: Unlike the conventional PK modeling which has descriptive significance, the PBPK modeling possesses the additional advantage of having predictive power. The accruing knowledge of the PBPK helps in risk assessment and uncertainty estimation.
- Aligned with the concept of personalized medicine: Knowing the physiological parameters and the pathophysiology in the diseased patients(or the physiology in the target patients), the pharmacokinetics and hence, the dosing information can be well established. Another application of PBPK is in personalized medicine. As an example, bariatric surgery leads to loss of absorption site from the stomach. Hence, the necessary dose adjustments can be estimated from PBPK modeling.
Opportunities entailing PBPK modeling
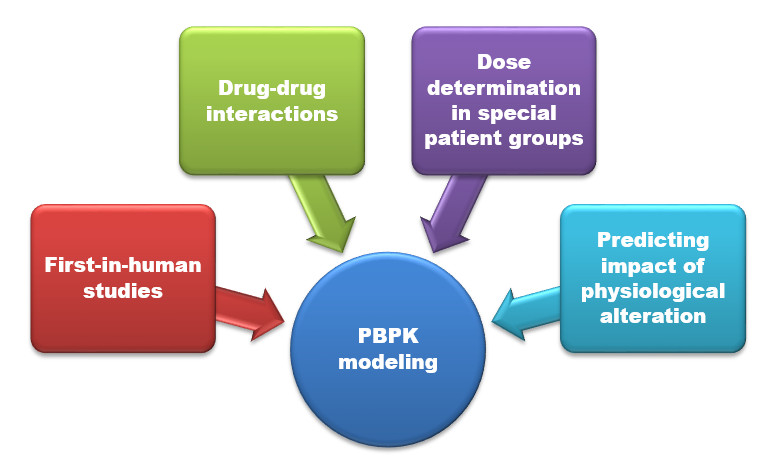
Pharmacometrics can influence every phase of the drug development process. It has the power to help develop new treatments for deadly diseases. PBPK modeling has established its niche that was previously unaddressed by the conventional in vitro and in vivo methods. Computation-based method bypasses the need to carry out tedious studies which are often associated with regulatory hurdles or applicability to the target patient groups. Figure 1 summarises the cases where the PBPK is applied. Regulatory authorities accept and even solicit the PBPK predictions in such scenarios.
An analysis by Mark Hovde demonstrated that pharmacometrics based modeling approaches can ensure the pharmaceutical industry to save nearly 97 million USD per new drug application (NDA). Savings are accrued through saving the number of patient requirement, time and increasing the probability of technical success. Improving the probability of technical success of just one percent is estimated to be worth 2 million USD per NDA.

Common Platforms of PBPK
PBPK models are dynamic models constructed using differential equations. Therefore, having a robust, efficient and reliable differential equation solver engine is an essential part of any software that deals with such models.
GastroPlus
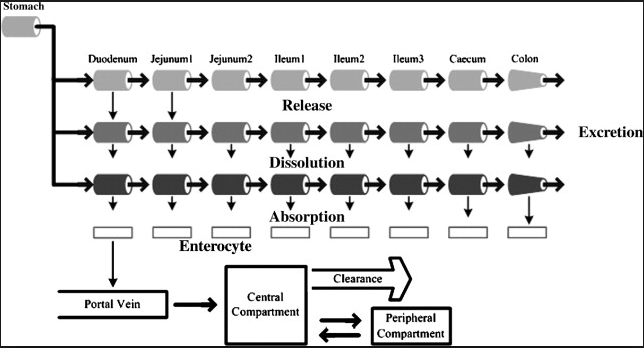
GastroPlus is a platform that is mechanistically based simulation software package that simulates absorption, pharmacokinetics, and pharmacodynamics in humans and animals. GastroPlus utilizes the Advanced Compartmental Absorption and Transit (ACAT) model (figure 2) for dissolution and absorption modeling.
Sensitivity to factors like pH, transporters, precipitation, paracellular absorption and others have been addressed quantitatively with the user being allowed to give the experimentally determined parameters as inputs. Population Simulator, Parameter Sensitivity Analysis and Batch Simulations modes enable the predictability in populations, parameter alterations and screening.

SimCyp
SimCyp population-based simulator aims to couple the population variability with PBPK to help explore potential clinical complexities prior to human studies and support decision-making in drug development. Simcyp Simulator users can conduct simulations in representative virtual populations. Simulating physiological variability enables predictions of drug disposition in relevant individuals with realistic variability. The ability to predict pharmacokinetic outcomes in the ‘real world’ patient populations is essential. To achieve this, our algorithms incorporate known variability in demographic and biological components within relevant disease populations.
Accounting for physiological variability is crucial to identifying individuals who are predisposed to the extremes of drug exposure prior to clinical studies. Linking drug-specific physicochemical and in vitro data on absorption and disposition in Simcyp algorithms allows prediction of drug behavior in the ‘virtual patient population’ as opposed to a ‘virtual reference man.’
PK-Sim
PK-Sim® uses building blocks that are grouped into Individuals, Populations, Compounds, Formulations, Administration Protocols, Events, and Observed Data. Building blocks from these groups are combined to produce a model. The advantage of building blocks is that they can be reused. For example, after having established a model for a drug after single-dose intravenous administration to an animal species, just substitute the individual by a suitably parameterized virtual human population and obtain a first in a man simulation model. Further substitute the formulation, to obtain a controlled-release per oral simulation model, substitute the protocol to obtain a multiple-dose simulation model, or substitute the compound to obtain a simulation model for another drug.
Others
MoBi® is a systems biology software tool for multiscale physiological modeling and simulation. Within the restrictions of ordinary differential equations, almost any kind of (biological) model can be imported or set up from scratch. Examples include biochemical reaction networks, compartmental disease progression models, or PBPK models.
However, de novo development of a PBPK model, for example, is very cumbersome such that the preferred procedure is to import them from PK-Sim®. Importantly, MoBi® also allows for the combination of the described examples and thereby is a very powerful tool for modeling and simulation of multi-scale physiological systems covering molecular details on the one hand and whole-body architecture on the other hand.
De novo model establishment and simulation is supported by graphical tools and building blocks to support expert users.
MoBi® uses building blocks that are grouped into Molecules, Reactions, Spatial Structures, Passive Transports, Observers, Events, Molecule Start Values, Parameter Start Values, and Observed Data. The different building blocks are described in detail in Part IV, “Working with MoBi®”. Building blocks out of the above-mentioned groups can be combined to generate models. The advantage of building blocks is that they can be reused. For example, a different set of starting values may define a new scenario, situation, or individual.
STELLA® is a powerful, graphic, object-based, model-building tool used to simulate various systems and processes.
PBPK in the Current Trend of Drug Discovery and Development
Aligned with the tenets of hypothesis-based drug development (also termed as Design-Make-Test-Analyse (DMTA) methodology) and the Model-Informed Drug Development(MIDD) Through its Critical Path Initiative (CPI), FDA advocates the development of methods that make the development process predictable and more effective. The goal of CPI has been described as a development of new, publicly available scientific and technical tools – including assays, standards, computer modeling techniques, biomarkers, and clinical trial endpoints – that can translate the effectiveness and safety profile of molecules in the earlier stages of the process.
FDA defined pharmacometrics as the science that quantifies drug, disease and trial information to aid efficient drug development and/or regulatory decisions. FDA’s Pharmacometrics integrates knowledge across the development program and compounds and biology while analyzing drug, disease and trial models with the special focus on drug models that describes the exposure-response relationship for therapeutic and side effects in light of individual patient’s characteristics. The models have been categorized as drug, disease and trial models.
While the drug models describe the exposure-response relationship for therapeutic and side effects in light of individual patient’s characteristics, the disease models compare the biomarker levels with the clinical outcomes and the time course of the disease and placebo effects. Trial models describe the inclusion/exclusion criteria, patient discontinuation, and adherence.
The primary aim of pharmacometrics is to aid decision making for approval and labeling of drug products with particular attention to drug dosing for all patients. It plays the role of consultant for advising sponsors regarding trial design decisions and conducts research on the available data for creating a new knowledge base and validate the existing disease models. FDA pharmacometrics has enlisted Design by Simulation as one of its 2020 Strategic Goals through which it aims to leverage prior knowledge to design Pediatrics Written request trials for 100% Pediatric Written Requests.
Model-informed drug development as defined by Richard Lalonde as “development and application of pharmaco-statistical models of drug efficacy and safety from preclinical and clinical data to improve drug development knowledge management and decision-making” has been identified by the FDA as an important way to help reduce attrition and uncertainty in drug development.
Even the FDA’s PDUFA VI goals intend to advance Model-informed Drug Development (MIDD) among other objectives in order to accelerate the approval process of safer therapies.
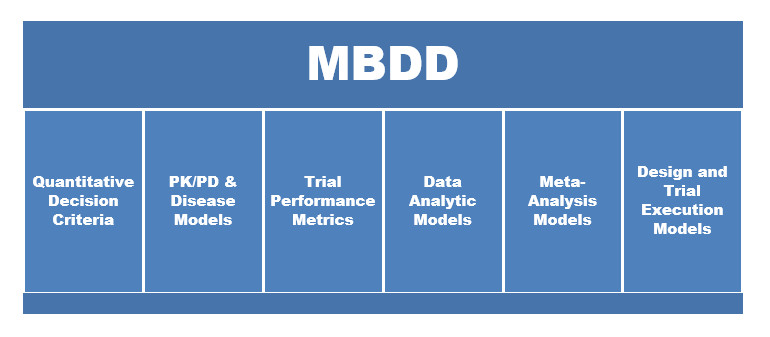
MBDD works on the paradigm of learn-predict-confirm cycles which integrate two or more of the six components (figure 3).

Conclusion
Drug development and regulatory decisions are driven by information that is compiled not only from clinical trials and supportive experiments but also through clinical experience in the post-market period. While the decisions are usually simple in nature (e.g., trial design and project progression at the company, product and labeling approval at FDA), the data informing the decision are complex and diverse.
Pharmacometrics or specifically, PBPK modeling has the potential to support the drug development process through model-informed decision making. This can ensue in huge savings in the form of lesser patients, saved time and increased probability of success. Various platforms are available commercially for pursuing PBPK modeling. Regulatory acceptance and soliciting of PBPK data by various regulatory authorities have brought pharmacometrics at the discussion center stage, allowing the industries to further invest in it. Future may see increased applications and approvals of drug based on PBPK modeling.
About the Authors


Ikjot Sodhi, PhD
Ikjot Sodhi has pursued her Ph.D. from National Institute of Pharmaceutical Education and Research (NIPER), SAS Nagar. She completed her B. Pharmacy from Panjab University and Master’s in Pharmaceutics from NIPER. She secured all India rank (AIR) 1 in GPAT 2011 and AIR 2 in NIPER-JEE 2011. She has worked in the domain of Pharmacovigilance for nearly two years. Having the research acumen and due awareness of the current regulatory obligations and lacunae, she writes to highlight the direction of growth of the Indian and global pharmaceutical industry.


Savitri Yadav, MS
Savitri Yadav has completed her MS(Pharm) in Pharmaceutics from National Institute of Pharmaceutical Education and Research (NIPER), SAS Nagar. She completed her B. Pharmacy from Panjab University. She is currently working as a Business Analyst at Evalueserve, Gurgaon, Haryana.
Disclaimer
The responsibility of the originality and usefulness of this content described above is of the authors and does not necessarily represent the views and policy of pharma mirror and its alliance. The authors also declared that they have no conflict of interest here.